One physician rose above early doubts about his future to become a department chair. Another physician returned to medicine after he was paralyzed during his residency. And prospective medical students with disabilities now have "a seat at the table." Throughout Michigan Medicine, people with disabilities are breaking down barriers and showing the world just how capable they are.
The patient tells his story with his hands, postures, and facial expressions: a rapid-fire set of movements that he uses to explain to his physician that he has continued post-surgical pain in his right foot, believes he is no longer able to work in a factory because of the pain, and fears living in isolation because he has so few people with whom he can communicate.
In the past, that feeling of isolation followed him to his doctors' offices. He would try to understand what the physician was saying to him, always through an interpreter. Sometimes the conversations went smoothly, but, more often, misunderstandings arose. Misunderstandings that led to confusion about one of his previous foot surgeries and made him wary of the entire medical community.
But on this day, the patient could not be happier with the care he is receiving from Michael McKee, M.D., assistant professor of family medicine and medical director of the Michigan Medicine Deaf Health Clinic at U-M's Dexter Health Center. "Dr. McKee really understands. I can talk right to him," he says through a medical scribe at the Deaf Clinic who also communicates in American Sign Language (ASL). "Dr. McKee's sign is so good. The best."
McKee's fluid and fluent signing has developed through a lifetime of communicating with ASL and being part of the Deaf* community. He has bilateral profound sensorineural hearing loss and uses a combination of a behind-the-ear hearing aid and a cochlear implant.
The Deaf Health Clinic is led by McKee and also includes Philip Zazove, M.D., the George A. Dean, M.D., Chair of Family Medicine, who is Deaf — and whom physicians once said would be lucky to grow up to be a janitor. The clinic is providing a vital service to patients from all over Michigan. More than 100 Deaf patients, and many others who are hard-of-hearing, go to the Deaf Health Clinic to receive accessible care, most for the first time in their lives. They are just a fraction of the millions of people in the United States who have significant hearing loss. The National Center for Health Statistics reports that approximately 20 percent of American adults (48 million) have some degree of hearing loss, a number that is increasing rapidly as people are living longer and experiencing age-related hearing loss.
"I think Mike and I are the only two physicians in Michigan who sign," says Zazove. "People come to us from all over the state. The communication barriers, especially when you're talking about mental health, are very difficult to overcome with patients who have hearing loss." He and McKee want to ensure that Deaf and hard-of-hearing patients can access and receive health care that is equal to their hearing counterparts' care.

The clinic is just one element of Michigan Medicine's inroads in the treatment of patients with disabilities, from deafness to mental health issues to paralysis. U.S. Census Bureau data show that one in five Americans has a disability, and barriers to quality health care arise at every turn: accessibility of physicians' offices, narrow parking spots, hard-to-read signage, conversations with health care providers, and more. Progress in clinical and research settings is occurring throughout Michigan Medicine, particularly in the Department of Physical Medicine and Rehabilitation and the Department of Family Medicine — thanks in no small part to physicians who themselves have disabilities. The U-M Medical School is also being recognized for its efforts in improving experiences for students with disabilities, with the goal of including those students and also of enhancing the experience of their classmates by providing them a more inclusive perspective.
Lisa Meeks, Ph.D. (Fellowship 2018), assistant professor of family medicine, was the co-investigator and lead author of a first-of-its-kind report released in 2018 by the Association of American Medical Colleges (AAMC) that explored the current state of medical education for medical students and physicians with disabilities. The report revealed common barriers to inclusion, as well as opportunities that will help enhance the academic medicine community's approach to students, trainees, and physicians with disabilities. These mechanisms will be more deeply explored in October 2020, when the U-M Department of Family Medicine hosts the inaugural World Congress on Disability in Medicine, bringing together researchers, educators, and health care providers from around the globe to address equal access to education, training, and improved access to health care for people with disabilities.
The department is working with the Coalition for Disability Access in Health Science and Medical Education to host the event, and partnering with the Medical School, the Department of Physical Medicine and Rehabilitation, the Office for Health Equity and Inclusion, and other schools and departments.
At the Department of Family Medicine Deaf Health Clinic, social worker Leslie Pertz, LMSW, an ASL-Certified Interpreter and licensed social worker, provides care to patients who have mental health issues. A medical assistant is committed to becoming fluent in ASL, a scribe already is fluent, and a front desk clerk can communicate with patients using sign. The team is finding ways to reach Deaf and hard-of-hearing people, especially in rural parts of the state, through telemedicine, including for mental health services. For Zazove, this isn't just about improving care for a single population. "We're a public university, and we need to take care of all of the people of Michigan," Zazove says. "It's the right thing to do."
The clinic's patients often say how they are receiving better care than ever before. The patient with the post-surgical foot pain, for one, feels fortunate to have the clinic in Michigan. "Four years ago, I started to see Dr. McKee, and my health has been better since then," he says. "I feel very supported to have someone who understands me."
Disabusing Disability
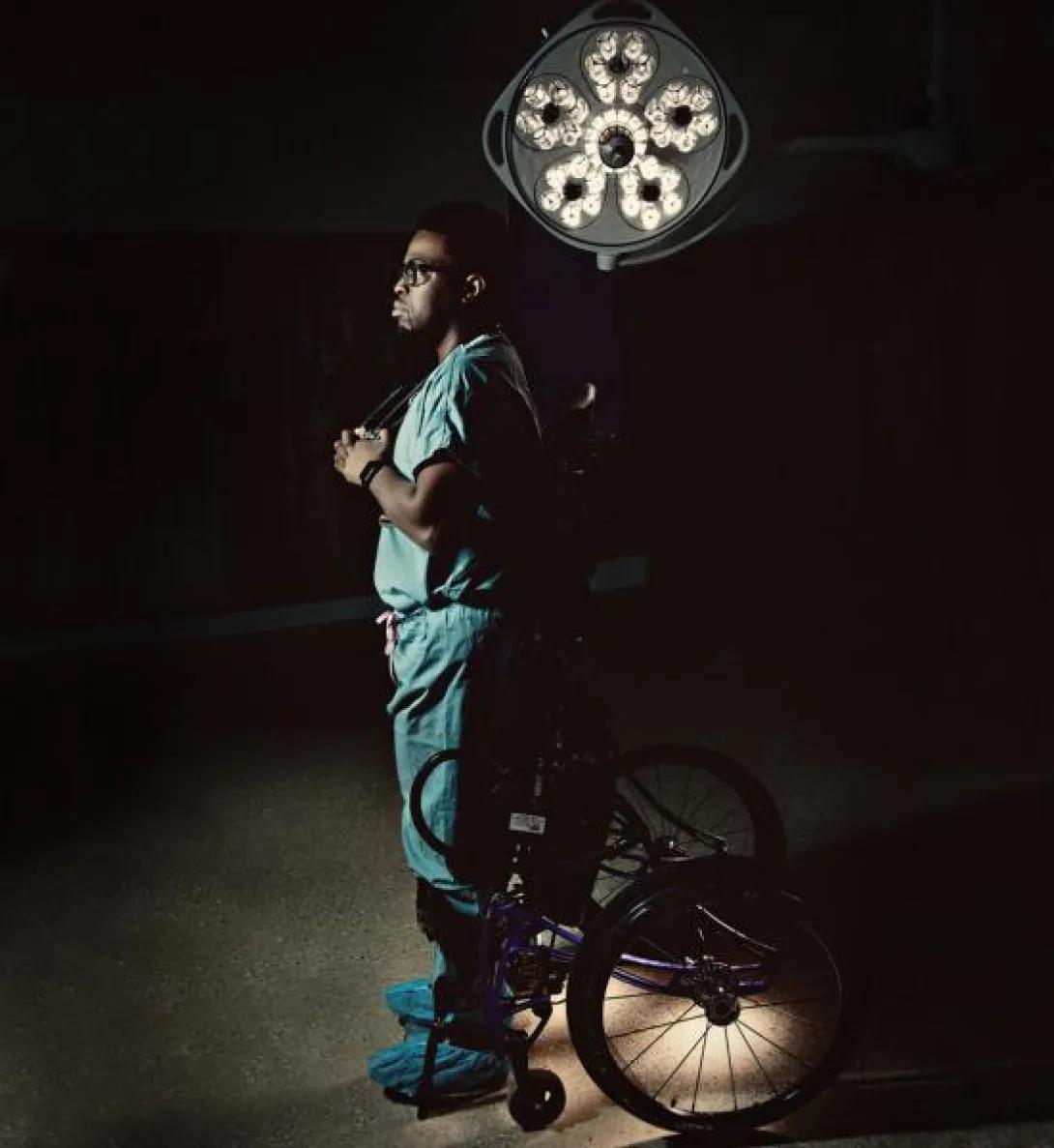
Feranmi Okanlami (M.D. 2011) — now an assistant professor of family medicine, and of physical medicine and rehabilitation — never thought, "I can't be a doctor now." He did not let himself spiral into despair or think about quitting. Nobody would have blamed him if he had, but anyone who has met Okanlami knows that giving up is not on his jam-packed to-do list.
The former Stanford track All-American was in the third year of his orthopaedic surgery residency at Yale when he attended a Fourth of July pool party in 2013. He jumped into the pool — just a jump, not a fancy dive or backflip — and the impact of hitting the bottom or side of the pool, or possibly someone's leg, left him immediately unable to move anything from his chest down.
Yet he knew, even in those early moments of his spinal cord injury and paralysis, that this was not the end to his lifelong dream. "I did not necessarily know how I was going to be able to get back to medicine and be a physician, but I believe in the verse Philippians 4:13: 'I can do all things through Christ who strengthens me.'"
Okanlami began to see that he would have an opportunity to demonstrate that having a disability doesn't mean people can't achieve their goals. He grew exhausted from inpatient and later outpatient rehabilitation near his home in South Bend, Indiana, but he never slowed down. Each day, with every assisted step on the treadmill, every range-of-motion stretch, every turn on the stationary bike, every surgery, he slowly learned to walk again.
Meanwhile, Okanlami earned a master's degree in engineering, science, and technology entrepreneurship from the University of Notre Dame; was appointed by South Bend Mayor Pete Buttigieg to sit on the county board of health; and coached the River City Rollers wheelchair basketball team. He transitioned to the family medicine residency program at Memorial Hospital in South Bend, where he reveled in the scope of the work. "I was able to take care of patients from cradle to grave — delivering babies, taking care of patients in nursing homes, and everything in between."
"I think parents of my patients see hope, see possibility, because they have met someone with a disability who is their physician." — Karin Muraszko, M.D.
In 2018, he joined Michigan Medicine. While some patients are unaccustomed to being treated by a physician with a physical disability, most of them adjust quickly. "As long as I'm able to demonstrate my complete competence in whatever it is that we are talking about that day, patients actually connect with me more," Okanlami says. "I think they often don't see the chair in the same way because they see me as human."
Surgeries and intense physical therapy have returned some function to his legs, to the extent that he is able to walk short distances with the use of forearm crutches. His hydraulic standing- frame wheelchair allows him to essentially stand while performing medical procedures. It also has given him insight into the ways he is viewed when he is in the chair. "When I'm seated, people don't expect as much of me — that I have a degree or the experience that I've had. I get more 'buddy' and 'pal' when I'm seated," Okanlami says. "I get a lot more 'sir' when I'm standing."
Okanlami's connection with patients who have physical disabilities is often instantaneous, he says. He and other physicians with disabilities "may be able to advocate for patients in a way that others may not have the ability to do, and we can have an amazing impact on the entire population of people we care for." One of those physicians has been a mentor to Okanlami: Karin Muraszko, M.D., chair and Julian T. Hoff, M.D., Professor of Neurosurgery, who has spina bifida and uses a wheelchair. Muraszko, a legend at U-M and the wider medical community, also is the first female chair of neurosurgery in the country. She specializes in pediatric neurosurgery. "I think parents of my patients see hope, see possibility, because they have met someone with a disability who is their physician," she says.
Okanlami also has taken on the role of director of medical student programs in the Medical School's Office for Health Equity and Inclusion (OHEI). He has adopted a catchphrase — "disabusing disability™" — on social media and beyond, with the intent of demonstrating that being disabled doesn't mean one is unable.
"Even as practitioners, taking care of individuals with disabilities is not something that most people are comfortable with," Okanlami says. "As we go into medicine, we are going to encounter people with different levels of function, and it's something we are not doing a good job preparing our medical students for: a world where you go into a room and your patient might come in a wheelchair, and then how do you address that? How do you get them onto the examination table? How do you perform your physical exam when the person can't lift their leg for you? A lot of people don't know how to treat you just because of a lack of knowledge — not because they don't want to, but because they just don't know how.
"And we don't talk about that to medical students. As a faculty member, I want medical students to know that it's OK to be human."

A Seat at the Table
When Molly Fausone and Chris Connolly applied to medical schools, they knew from the start that not all application processes were equal, and that not all schools would welcome them. They both discovered that many programs had technical standards requiring students to perform physical tasks such as lifting a patient. Fausone and Connolly both use wheelchairs due to paralysis in their legs, so this simply wouldn't be possible.
Technical standards vary by institution. Their purpose is to ensure a uniform set of attributes among enrollees. At many schools, these standards have not changed since 1979, when the AAMC issued recommendations for a universal skill set among applicants to ensure success in any specialty. "Many of them might not be consistent with the current interpretation of the law, frankly," says Rajesh S. Mangrulkar, M.D. (Residencies 1997 and 1998), the Marguerite S. Roll Professor of Medical Education, associate professor of internal medicine and of learning health sciences, and associate dean for medical student education at the U-M Medical School. "Legal experts say some of these wouldn't pass muster under the Americans with Disabilities Act."
Fausone found U-M to be welcoming and encouraging. Connolly applied after the school revised its technical standards in 2016 to include students with a physical disability or functional limitation, as long as alternative or supplemental means can help them learn the required hands-on coursework. In addition to physical and chronic health disabilities, the school can accommodate students with learning disabilities (such as dyslexia), mental health conditions (such as anxiety or depression), and ADHD by offering extra time on exams or a testing environment with limited distractions.
The move reflects the true aim of medicine and medical education, says Steven Gay, M.D. (Fellowship 1997), assistant dean for admissions and associate professor of internal medicine. "As physicians, we don't turn anyone away; our responsibility is to address every individual. By the same token, there is no substitute for learning with people who are different from you.
"Everyone needs to have a seat at the table."
Fausone has experienced that seat-at-the-table mentality. She was accepted at many medical schools, "but Michigan is the only school that reached out to me and said, 'You're a good fit; let's see how we can make this work.'"

The change in perspective is a useful one, not just for medical students who have disabilities, but for their peers, patients, and others, says Meeks, one of the country's top researchers in this field. "We teach that to be disabled is a bad thing. The point of medicine is to fix the problem," Meeks says. "We need to change that perspective, within the medical community and in our treatment of patients."
Fausone has thrived at Michigan, as has Connolly, an M2. Fausone, an M3, points out that she has needed few accommodations — mostly extra time for tests and a few equipment modifications. Muraszko taught her skills such as how to scrub in before surgery. She also thinks her presence as a medical student helps to normalize disabilities among her peers, and to strike down the divide between physician and patient. "Being a patient is a role," she says, "not an identity."
Clarissa Love, a project associate manager with OHEI, points out that "every one of us has multiple identities: race, gender, sexual orientation, age … disability is just one part of that identity, and it's one that isn't always visible to your colleagues." Love has helped spearhead the Michigan Medicine Disability Council, a group that focuses on disability awareness and advocacy for patients, faculty, staff, and learners. The council's goal is to "increase awareness and promote a system in which every program and department works together to adequately support the needs of our community members with disabilities," says David J. Brown, M.D. (Residency 2003), associate vice president and associate dean for health equity and inclusion, and associate professor of otolaryngology–head and neck surgery.
Not all disabilities are physical. Rahael Gupta, now an M4 at Michigan, had always thought of herself as optimistic and fun-loving — until her depression grew so debilitating that she thought of stepping in front of a bus one night.
The incident prompted her to take a seven-month break from medical school in 2016 to receive therapy and medication. She did not know, however, how much of her personal story she should communicate in explaining her résumé gap. Many well-meaning faculty members suggested she vaguely cite health problems. "As an aspiring physician, I may be committing self-sabotage by telling my story," Gupta wrote in a 2018 JAMA editorial. "I admit openly that I am just as vulnerable to the elements of life as are my future patients, hoping that others will do the same."
Gupta's experiences inspired her to create a project and accompanying video called Physicians Connected, which encourages an open discussion in the medical community about mental health conditions among students and practitioners. "If I have learned anything after spending most of my short life in pursuit of academic distinction, it is that the appeal of the dividends — good grades, high praise, awards — is as ephemeral as the warm glow felt on their receipt," she wrote.
"Not so with the call to protect human life; that's something truly worth living for."
Kevin Joy contributed to this story.
*This story uses the terms Deaf and deaf to mean, respectively, someone who self-identifies as Deaf or hard-of-hearing; and someone with hearing loss who identifies with the hearing world. The distinction is widely used among people who have hearing loss.
Read the stories of physicians from around the world who have disabilities by searching Twitter and Instagram for #DocsWithDisabilities, a social media campaign from the Michigan Medicine Department of Family Medicine that was co-created by Lisa Meeks, Ph.D., assistant professor in the department.

The World Health Organization's International Classification of Functioning, Disability, and Health (known as the ICF) is a widely used system for determining whether someone has a disability. The classification system measures people's difficulty with cognition, mobility, self-care, interacting with other people, life activities, and participation. "We have a societal norm, and if you have a level of functioning that challenges your ability to function in society, you have a disability," says Edward A. Hurvitz, M.D. (Fellowship 1989), the James W. Rae Collegiate Professor and chair of the Department of Physical Medicine and Rehabilitation. Self-perception also plays a role. Hurvitz sees patients with spinal cord injuries who say they don't have a disability "because they are able to function perfectly well in society." Other patients have less-severe injuries or conditions but have a disability because they are not able to function well in society, he says. "There is not a single standard that applies to everybody."
What happens when a person with a physical disability ages? How do his or her needs change? What is it like to manage conditions like diabetes when you're already living with a spinal cord injury or cerebral palsy?
"It adds another level of complexity," says Michelle Meade, Ph.D. (Fellowship 2000), associate professor of physical medicine and rehabilitation. With that in mind, Meade sought funding from the National Institute on Disability, Independent Living, and Rehabilitation Research to establish a Rehabilitation Research and Training Center (RRTC) program at U-M. She and her team received the five-year, $4.3 million funding in 2018.
"My ultimate goal is to make it easier for folks who are aging with a physical disability to do so. We hope the RRTC serves as the infrastructure and backbone for continued focus on collaborative research and community interaction," she says.
Known as the Investigating Disability Factors and Promoting Environmental Access for Healthy Living RRTC — or IDEAL, for short — the U-M center will use the research it generates to develop evidence-based interventions to help this patient population live better. "I wish more health care providers were aware that people with disabilities are working hard to make their best life possible," Meade says. "They encounter many challenges in trying to make that happen." The IDEAL RRTC has four main objectives:
- Identify environmental factors — including practices, programs, and policies — that are associated with healthy aging for individuals with long-term physical disabilities from diverse backgrounds, particularly those from low-income and racial/ ethnic minority communities.
- Develop interventions to modify environmental factors to enhance the health, functioning, and participation of individuals aging with long-term physical disabilities.
- Serve as a national resource center to improve outcomes for people aging with long-term physical disabilities, their families, and other stakeholders by providing information, training, and technical assistance to a variety of groups — including individuals with disabilities, disability and rehabilitation researchers, clinicians and service providers, and policymakers.
- Engage key stakeholder groups, particularly disability- and aging-related organizations, to bridge programs and practices for older adults and people with disabilities, and maximize the relevance and usability of the knowledge generated by the RRTC.
"We don't want people with disabilities to always have to ask more questions and do more research," Meade says. "How do we make it so it's not entirely up to them to make things better?" The IDEAL RRTC is led by Meade and her co-principal investigators, Philippa Clarke, Ph.D., professor of epidemiology at the U-M School of Public Health, and Robyn Rontal, J.D., MHSA, policy analytics director for the Center for Healthcare Research and Transformation in Ann Arbor. "The center is truly leveraging what's best about U-M: partnering with our colleagues and communities to make a difference," Meade says.
New Horizons
The IDEAL RRTC is one element of the robust research being conducted throughout Michigan Medicine regarding disability health. Topics include the health outcomes of pediatric-onset disabilities across the lifespan, accessibility in medical education, neurogenic bowel and bladder issues, contraception and reproduction, the health literacy of people who use hearing aids, the development of adapted devices that assist physicians and other care providers who have disabilities when they are treating patients, and much more. Read more in our 2019 feature on disability.
Kylie Urban contributed to this report.
Featured News & Stories
The Race to Uncover the Hidden Causes of Idiopathic Pulmonary Fibrosis

Shipt gift helps address food insecurity

Giving with gratitude: planned gifts support nursing, research, and patient care
Addressing Senior Social Isolation in the Community
The Impact of Social Isolation and Loneliness on Cognitive Health
