Children's Mental Health Is in Crisis
Here are 7 things we can do right now to help.
Author |

"People are calling me, saying, 'I and my child have been in the ER for a couple of days now, waiting for a bed. My child is suicidal. We can't go home … and I'm terrified. What do I do? How can you help?'" says Donna Martin, M.D., Ph.D., chair of pediatrics, the Ravitz Foundation Endowed Professor of Pediatrics and Communicable Diseases, and professor of human genetics.
"And that's just wrong."
The situation is severe. But it is not new.
"We were shouting from the rooftops, saying we are in crisis," says Emily Fredericks, Ph.D., professor of pediatrics and director of the pediatric psychology division at Michigan Medicine. "There are not enough mental health providers to meet needs of children in our state. We knew we were in a dire situation.
"The pandemic has exacerbated that. Infinitely."
"I've said it so often it sounds trite," says Gregory Dalack, M.D., the Daniel E. Offutt, III Professor of Psychiatry and chair of the department. "All these needs were there. The pandemic has really just squeezed the vise on the system."
That squeeze prompted an unprecedented event last fall when the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, and the Children's Hospital Association declared a national emergency in child and adolescent mental health.
"We have thousands of patients waiting to get access to child psychiatric ambulatory services within our health system and in the community," says Nasuh Malas, M.D., associate professor of psychiatry and of pediatrics and service chief for child psychiatry at C.S. Mott Children's Hospital. Malas and his colleagues published a study in Clinical Pediatrics in January showing an 18% rise in initial psychiatry consults at Mott from July 2020 to January 2021 compared with the 2019-2020 time period. This is a four-fold increase in mental health consultation demand compared with the rate of increase from previous years.
And it's not just the sheer volume of demand that has increased, but also the acuity of distress for individual patients. A Michigan Medicine study published in Clinical Child Psychology and Psychiatry in March shows that pediatric patients receiving psychiatry and/or psychology services during the pandemic were more likely to require restraints and antipsychotics than those treated just before the pandemic. "We used to see middle-of-the-road severity," says Fredericks. "Now every patient worries me."
We have a tsunami of need across the country, and we have little more than sandbags to meet it.
As with natural disasters, there are heroes of this crisis — both visionaries who have seen this coming and have spent many years preparing, as well as those who have been called to action at this sharp pain point. But according to the myriad mental health experts interviewed for this article, what is needed even more than individual heroes is broad systemic change.
Below are seven actions that we in health care and as a country can take to help alleviate this crisis. Most of these are already underway at Michigan Medicine — at C.S. Mott Children's Hospital, the Nyman Family Unit for Child & Adolescent Mental Health & Wellness, the Eisenberg Family Depression Center, and the many clinics that address children's mental health.
1. Train More Providers
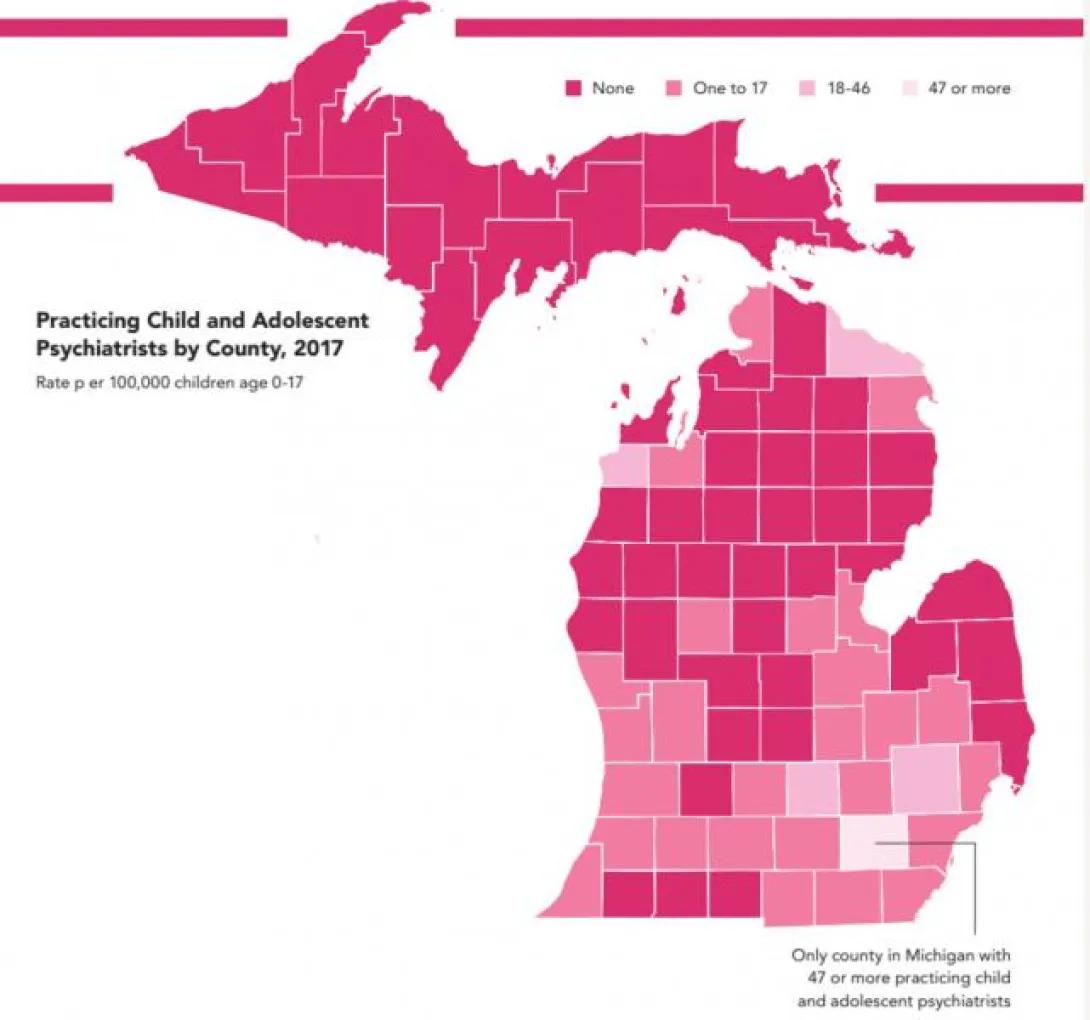
"The number of child psychiatrists has always been tiny, miniscule — never anywhere close to a reasonable number for the population," says Laura Hirshbein, M.D., Ph.D., professor of psychiatry, who is also a historian currently writing a couple of books on the history of children's mental health. In Michigan, only one county (Washtenaw) has an adequate number of child and perinatal psychiatrists.
Historically, "child psychiatrists were pretty poorly paid among medical specialties," says Sheila Marcus, M.D., professor of psychiatry. "And at the end of five years of training following medical school, these early-career physicians had difficulty with student loans." The Michigan Department of Health & Human Services now has a loan repayment program for mental health care providers who spend two years working at a non-profit health clinic in health profession shortage areas or in child and adolescent psychiatry hospital-based settings.
"We are training more pediatric psychologists," says Fredericks. "[But] there is more interest than there are spots available. On a national level, there is advocacy going on to increase federal funding for training child and adolescent psychologists." However, we are still far from where we need to be. "As a health system, we need more investment in psychologists," says Martin. "We could easily have four times as many psychologists as we do right now, and still not have enough."
"What we do have now that we didn't used to have is that pediatricians are taking on the role of becoming primary mental health providers," says Hirshbein. Most prescribing of psychiatric medications for kids is done by primary care physicians. "Families like to be treated in primary care because they have comfort with their doctor and because of the issues around stigma," says Marcus. "The question is, 'How can we spread out expertise so that people know what to do [when families come to them with mental health concerns]?'" says Hirshbein.
One answer is the Michigan Child Collaborative Care Program (MC3). Marcus founded the program ten years ago, when she saw how difficult it was for primary care physicians to meet the growing demand for psychiatric care. MC3 partners with the Michigan Department of Health & Human Services to support PCPs who are responding to mental health crises.
When a primary care provider initiates a consult with MC3, a behavioral health consultant triages the request, responding to questions within the scope of their expertise and forwarding appropriate cases to a psychiatrist at Michigan Medicine for same-day phone consultation. In many cases, the behavioral health consultant will also identify local resources for the patient.
MC3 has been able to leverage the psychiatric expertise of a handful of psychiatrists at Michigan Medicine to meet the needs of children and women across the state. As of March 2022, MC3 has enrolled 3,100 providers, helped 16,000 patients, and provided 38,000 services.
The MC3 Program is also one of several in the country that has a thriving perinatal consultation program, providing consults to primary care physicians caring for women during pregnancy and postpartum. "When mothers with depression and trauma are identified early, it makes it possible for consultants to guide them toward infant mental health specialists who help foster healthy, secure attachment relationships with their babies," says Marcus. "This early bonding helps ensure a healthy developmental trajectory for infants from the start."
MC3 has also given primary care providers continuing education in mental health care, through its educational modules on topics like eating disorders, ADHD, and other mental health issues. Training these providers to become better mental health caregivers is one way that MC3 has helped to increase the number of providers who can meet the demands of the crisis.
2. Innovate to Increase Access
Mental health concerns are common. About 1 in 5 children has a diagnosable mental health condition, but only half of them get proper care. Though holistic medicine and whole-person care are widely accepted and generally touted as important, mental health care is too often siloed in specialty practices that remain inaccessible for many families.
"We need to make sure mental health care is accessible to everybody in the way that physical health care is accessible," says Joanna Quigley, M.D., associate professor of psychiatry and of pediatrics, as well as associate medical director of child and adolescent ambulatory psychiatry services. "It should be just as easy as accessing a primary care provider for a well-child check."
This is an area where the broader health care community could use large health systems like Michigan Medicine as a role model. At C.S. Mott Children's Hospital, psychology and psychiatry services are fully integrated into children's medical care. "Having psychologists integrated where kids are getting care provides better care and better access," says Kristin Kullgren, Ph.D., associate professor of pediatrics.
"We're thinking about how we can be more thoughtful about integrating care, embedding mental health professionals in medical settings. We're working with medical providers to ensure we're screening early and providing preventive services," says Malas, who directs the psychiatric consult service at Mott.
Another innovation that has improved access to mental health care is telehealth. It's hard to believe that just two years ago, telehealth was relatively rare. "Pre-pandemic, I did a total of one virtual visit with patients," says Kullgren. But now she is a big proponent of telehealth, especially for children's mental health. "For me and my patients, there are a lot of positives to virtual care. Access is huge for kids. They can log on from home, from school, the McDonald's parking lot, wherever they happen to be, and I can give them care. Whereas before, what used to take half a day or a day to come to the appointment, now takes just the appointment time."

In addition to integrating mental health care with medical care and continuing to expand access to mental health care via telehealth, we also need to think of innovative ways to relieve the current pressure on psychiatric emergency services.
Right now, psychiatric beds for children are at 95% capacity at the Nyman Family Unit, says Malas. "At any given time, we may have 6 to 8 kids in our health system waiting on a psychiatric bed." Some may wait for several days.
The answer is not necessarily more beds. "We need to get care to patients locally and early in way that is feasible, sustainable, and natural, rather than having people coming to ER in the middle of the night in crisis," says Malas. He also recommends expanding mental health services "so it's not just an outpatient/inpatient model." He says we need urgent care centers that are equipped to handle mental health issues, respite centers for adolescents who need a cooling-off period, and partial hospitalization programs.
Malas and Quigley are part of a group that is developing a partial hospitalization program for children and adolescents. A program like this could provide intermediate-level psychiatric care, similar to the partial hospitalization program that already exists for adults.
"We have to shift our framework to not think about mental health care as something that only happens at a psychiatric clinic," says Quigley. "We need to integrate this care into all aspects of the health care delivery process."
3. Improve Insurance Coverage

For many families, having access to mental health care is almost synonymous with having insurance coverage. But from an insurance standpoint, mental and physical health are not treated equally. "Insurance companies have turned toward very aggressively managing mental health care to make providers show that someone really needs it, in a way that they don't with other illness," says Hirshbein.
"From a purely insurance-based perspective, we need federal regulatory changes," says Jack Kaufman, Ph.D., an associate professor of physical medicine and rehabilitation who conducts neuropsychological testing for children, which, like all other mental health services, has seen an increase in demand. "We need to not have insurance companies telling us how many units of something they're going to give us to solve it before we even [have a diagnosis]."
Kaufman also says we need to make sure the same services are reimbursed by insurance at the same rate — regardless of who provides the service. For example, she says a psychotherapy session might get reimbursed at a higher rate for a physician than a psychologist, even though conducting that kind of session does not require a medical degree. "There are services that I, as a psychologist, can't do that cost more, and that makes sense. But the service should be charged the same, if it's the same service."
Making this change to insurance reimbursement could incentivize the hiring of a broader range of mental health care providers to meet the demands for psychological services.
We also need to make it easier for mental health care providers in the community to be covered by insurance. One reason that large health systems, like Michigan Medicine, have such long waitlists is because they are often the only recourse for families who cannot afford to pay out-of-pocket for mental health care.
4. Learn More about Kids' Brains
"The period of preadolescence through adolescence into early adulthood is really when mental health problems emerge," says Mary Heitzeg, Ph.D., professor of psychiatry. "It's also when the brain is going through critical developmental processes."
She and Chandra Sripada, M.D., Ph.D., associate professor of psychiatry, are principal investigators in the Adolescent Brain Cognitive Development Study (ABCD). The groundbreaking nationwide study includes 21 sites where data is being collected on 11,800 youth (720 of them are enrolled at Michigan Medicine). Before this study began six years ago, a really impressive sample size for a study like this would have been 100, says Heitzeg.
Every year, each of the enrolled youth and one of their parents undergoes an eight-hour assessment. That includes neurocognitive tasks as well as a sizable set of questionnaires that glean data on everything from sleep quality and substance use to screen time and extracurricular activities. At baseline, and every other year afterwards, the assessment includes fMRI to record brain changes. Researchers also collect data at the midpoint of each year.

But how can simply having all of this data improve children's mental health?
That's where another technological advancement comes in: data sharing. Data from the study is accessible to researchers around the world, and some 400 studies based on ABCD have been published so far, says Sripada. The richness of the data set allows for an astounding array of interpretations that could have profound implications for kids.
"One of the things that ABCD has helped us to definitively establish is that socioeconomic factors — resources of the household, income relative to needs, neighborhood disadvantage, and parental education — have big effects on kids' brains, in the brain structure, in connectivity patterns, and in the ways the brain responds to tasks," says Sripada. "This might have some policy implications."
Heitzeg points out that the longitudinal nature of the study will also allow researchers to see the outcomes associated with these brain changes. "Are they more at risk for mental health problems, doing worse in school, etc.?"
Heitzeg says another richness of the study is that "we have all this other info. For example, organized sports. We can, in theory, have a group of kids with the same socioeconomic status and same brain changes, but they're in sports and another group is not. We can see how a potential protective factor like [sports] may moderate the outcome."
"The last piece of the puzzle is the influence of macro-environmental events, for example, COVID-19, or the profound and long-term impact of major wartime disaster, like that in Ukraine," says Robert Zucker, Ph.D., active emeritus professor of psychiatry and psychology, director emeritus of the Michigan Medicine Addiction Center, and one of the original principal investigators on the ABCD study.
Zucker has had a career-long interest in the causes and treatment of mental health problems and conducted a study on the origins of behavioral problems and substance abuse in children to examine these questions. The study ran for 31 years, beginning in 1985 with children ages 3-5, the earliest developmental age that had ever been studied in this way. It also included data on those children's parents, and Zucker says it has been the longest running study of the family interactional matrix and how it might contribute to the development of these problems or protect against it.
Zucker stresses the importance of understanding that the effects of major historical events on the health of a generation are probably an interaction with the mental health adaptation and the social resources of the youth experiencing those events. ABCD investigators have understood this, too. When the pandemic began, he says, ABCD researchers pivoted quickly to include questions in their assessments about the effects of COVID-19 on families. That study is already tracking those effects over time, and early results show such interactions.
"Most mental health problems and concerns are long-term and chronic," says Zucker. "They remit. But a cure — a complete cure — is relatively rare. The solution to that from a public health standpoint is to prevent. The detailed knowledge obtained by ABCD has the potential to identify what the targets need to be for this long-term prevention."
5. Prevent Mental Illness
What is the ideal age to begin helping kids in order to promote mental health and prevent mental illness? At Zero To Thrive, the answer is before birth.
Housed within the psychiatry department, Zero to Thrive delivers mental health services to individuals and families from conception through early childhood.
"The science is clear: brain development in the earliest years lays a critical foundation for later well-being, and intervention to promote early relational health has demonstrated a strong return on investment," says Maria Muzik, M.D., M.Sc., co-director of Zero to Thrive and associate professor of psychiatry and of obstetrics and gynecology. "Effective programs need to address critical mental health needs not only through access to psychiatric care, but also by reducing the social isolation that so many families experience, supporting parents in meeting their own and their child's emotional needs, and connecting families to resources in the community to meet the full range of family needs."
Zero to Thrive teaches the importance of early relational health and what it looks like to build a responsive relationship between a caregiver and an infant. When caregivers are positive and responsive, a baby's brain gets the stimulation needed to form the neural pathways to build resilience and thrive. Trainees at the Medical School work in both a perinatal clinic that serves pregnant and postpartum people, and in the Infant and Early Childhood Clinic that serves families from birth through age 6 using cutting-edge video-observation and feedback technology to support and nurture family strengths.
"While our clinic-based services are critical, if we wait for families to reach us in psychiatry, we will have only reached the tip of the iceberg," says Katherine Rosenblum, Ph.D., co-director of Zero to Thrive and professor of psychiatry, of pediatrics, and of obstetrics and gynecology. "That is why we place a great deal of emphasis on partnering with community providers, offering training to multidisciplinary providers in perinatal and early childhood mental health, and thereby reaching families where they already are — from pediatric primary care, to early care and education, to other community-based programs."
A key part of Zero To Thrive is a series of Strong Roots programs that help kids by building resilience in families, especially those who have been exposed to adversity such as trauma, economic oppression, or inequity. Studies of these programs have demonstrated positive impacts for both parents and children, including improved early relationships, changes in parental brain circuitry that are associated with reduced parenting stress, increased social connection with other parents, and increased utilization of community services. There are programs for moms ("Mom Power"), dads ("Fraternity of Fathers"), and military families, as well as a program for early childhood educators who work with infants and children in preschools and nurseries. Zero To Thrive has trained professionals who are rolling out these programs in community-based organizations all over the country. Zero To Thrive also conducts research, education initiatives, and a clinical enterprise to help pregnant and postpartum people with mental health issues.
"Schools, primary care providers, and local community resources need to find ways to integrate mental health and well-being in everything they do," says Malas. "We need to see mental health as a shared responsibility of all professionals who interface with children and families."
Another program started at Michigan Medicine that takes that integrated mental health model to heart is TRAILS (Transforming Research into Action to Improve the Lives of Students). TRAILS equips school staff with the training, resources, and clinical tools necessary to implement its three tiers of programming: 1) Social and emotional learning to promote resiliency and build students' self-regulation skills, and self-care strategies for staff to counter stress and burnout; 2) Early intervention for students with mental health concerns; and 3) suicide risk management and care coordination for students in crisis.
Studies show that students who receive the cognitive behavioral therapy and mindfulness training offered by TRAILS demonstrate a 16.9% decrease in symptoms of depression and/or anxiety, as well as an increased use of self-regulation and coping skills.
The Eisenberg Family Depression Center also offers a Peer-to-Peer program that began in 2009. The program educates middle and high school students about depression and depressive illnesses and helps them find creative ways to convey this knowledge to their peers. The program received the American Psychiatric Association's Gold Award for academic programs in 2019.
6. Help the Helpers
Attending to the needs of mental health care providers is a key component of protecting children's mental health.
A small change that could help these providers is to increase understanding of the many mental health specializations. "Would you send someone with a tummy ache to a dermatologist?" Kaufman asks. She often receives inappropriate referrals because referring providers are not aware of the full range of subspecialties within psychology and where to go for a given concern. For example, the neuropsychological testing that Kaufman does targets primarily cognitive concerns and diagnostics as opposed to behavioral or mood treatment, but someone might assume that she handles patients with those latter concerns because she is a psychologist. It's not just that it's frustrating to get an inappropriate referral, but it is an inefficiency in the system of mental health care that, if corrected, could free up specialized providers to offer the right care to the right patient at the right time.
A bigger challenge is offering better support to providers. "The mental health of the mental health providers is really low right now," says Kaufman. "We're the people who listen to everyone in crisis."
At the beginning of the pandemic, she and other mental health care providers at Michigan Medicine banded together to support frontline health care workers. There were 200 volunteers who provided in-person and virtual counseling to their Michigan Medicine colleagues who were seeing the worst of the pandemic. They also helped to educate them about the way trauma affects mental health and what they might expect to experience over time.
Now those volunteers are the ones experiencing an enormous burden, as the demand for mental health care far outstrips the supply of providers. Kaufman believes a meaningful first step towards helping mental health care providers would be to honestly acknowledge the ways they are suffering. "Appreciation is [best] shown by listening and hearing and being engaged in what's happening."
7. Change the Conversation
In the late 1960s, Congress commissioned a study that resulted in a report called Crisis in Child Mental Health. Hirshbein says, "It called out things like systemic racism, [showing] there's no way poor black kids can survive and thrive if living in these conditions. What's striking about this report is there's nothing in it about psychiatric diagnoses or medication.

"Child psychiatrists at the time were mostly psychoanalytical, but they were also activists," says Hirshbein. "They wanted government to do things to help kids. They were about big social changes." The Crisis in Child Mental Health report was initiated under President Johnson's administration, "but it landed on President Nixon's desk, where it promptly died." There were no big social changes coming.
Then, in the 1990s and 2000s, psychiatric medications for children became more accessible and commercialized, says Hirshbein. "The idea of diagnosing, treating, and focusing on mental illness was really a shift for child psychiatry. Yet the numbers of kids who are meeting criteria for mental illness are not going down. Something is happening, and we're going in the wrong direction."
Hirshbein believes it could be helpful to shift the conversation back to the question guiding the 500 experts who worked on the Crisis in Child Mental Health report: "What does it mean to raise a child to be healthy?"
One answer to that question involves helping kids learn basic social skills and rules of civility, assets Martin sees as casualties of the pandemic. "The skills we need to function as a society are under threat now," she says. "We've lost the social fabric of our community interactions, and Zoom is not a replacement for in-person communication."
Martin believes the isolation caused by the pandemic is especially fraught for children, who are just learning how to be social. She also worries about the increasingly uncivil tone of online discourse. "How do we course correct in a society where being vitriolic or accusatory or, frankly, abusive becomes the norm?
"If you're a child growing up in this environment, I worry about what you're going to look like 10 years from now. It's really scary. How do we create those meaningful interactions for families, individuals, and communities?"
A positive of the pandemic has been a shift in public conversations about mental health. "We've come a long way in addressing the problem of stigma in mental health," says Martin.
"I think it's great that we've declared this mental health crisis and that it's been acknowledged by several professional organizations and in the State of the Union address," says Quigley. "But this was brewing long before COVID-19, and I hope it continues to sustain people's attention and investment, because this is not going anywhere. There will be a generation of kids impacted by COVID-19 who will have needs ongoing. I think about my 3.5-year-old … COVID-19 is the life she remembers. The repercussions will be felt for a long time."
Featured News & Stories

Processed foods may be fueling the rise in binge eating

Alcohol-Related Liver Disease clinic gives patient new hope
Addressing Senior Social Isolation in the Community

Permission to Flourish: Well-Being for High Performers with Shigehiro Oishi

What’s the equivalent of a wheelchair for a person with schizophrenia?