A method to prevent falls before they happen
Fall prevention is typically discussed after the first fall, but one researcher is changing that with the JEDII method
10:34 AM
Author |
The risk of a fall is typically discussed with patients after they have experienced a fall or report poor balance.
For researcher James Richardson, M.D., a Professor of Physical Medicine and Rehabilitation at University of Michigan Health, this approach seemed backwards.
Richardson set out to create an in-clinic strategy at his JEDII Fall Clinic, or Judicious Early Detection of Impending Imbalance, to assess patients at risk of a fall and determine what steps need to be taken to prevent falls before they start.
Prior large-scale research shows that patients who can’t stand on one foot for 15 seconds or longer are at a much higher risk for falls within the next seven to 10 years.
To determine why a person’s stance time is less than optimal, Richardson created a series of tests to widely assess a patient’s fall risk.
One test includes a device created by Richardson called the ReacStick.
The science behind the method
The standard in-clinic assessment for fall risk prior to a fall is unipedal stance time, also known as UST.
This is the recommended measure of balance and fall risk in older adults, determining how at risk a patient is of falling by having them attempt to stand on one foot for 15 seconds.
However, this test doesn’t measure why, precisely, people cannot perform unipedal stance time for more than 15 seconds.
Richardson and team performed extensive research to determine which three tests best predict a patient’s fall risk.
Published in Aging Clinical and Experimental Research, the study included 172 participants.
Of those participants, 31 had varying degrees of diabetic neuropathy, 94 had varying degrees of cirrhosis without covert hepatic encephalopathy and 47 were older adults without known disorders.
All categories of participants are typically classified as someone at risk of a fall.
After analyzing the results, Richardson and team found that peripheral afferent function, central processing speed and frontal plane strength as estimated by these three clinical tests predict about two thirds of the variability seen in unipedal stance time.
These tests help patients understand why they cannot perform unipedal stance time for 15 seconds and why they are at risk for repetitive falls.
3 tests that measure for fall risks
Clinical vibratory perception test
For the clinical vibratory perception test, a vibrating tuning fork is placed on the nailbed of a patient’s large toe.
The patient is asked to inform the provider when they can no longer able to feel the vibration of the tuning fork.
The test aims to detect subtle changes in the peripheral nerves in the patient’s foot and ankle that could contribute to them being unable to quickly detect a trip or stumble, which could lead to a fall.
“The longer the patient feels the vibration, the better their ankle inversion and or eversion proprioceptive precision,” said Richardson.
“Ideally, the patient can feel the tuning fork on their foot for eight to ten seconds or more.”
The ReacStick
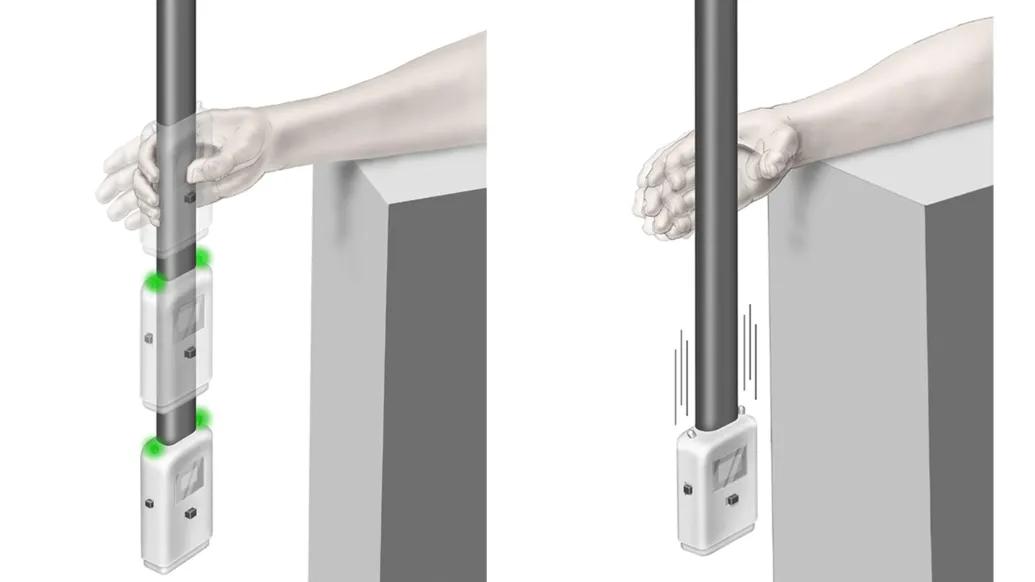
The second test uses a tool called the ReacStick.
Created by Richardson and his team at U-M Health, this device is just under the length of a yard stick with a monitor attached to the bottom recording the milliseconds between the device being dropped by the provider and caught by the patient.
Patients sit in a chair with their elbow resting on a desk or other flat surface in a position that allows their hand to be off the desk.
The patient will have a few practices to become familiar with how the ReacStick works.
Once the practice rounds conclude, the speed at which the patient catches the ReacStick after it has been dropped by the provider is recorded to conclude the patient’s Simple Reaction Time over the course of ten trials.
“The monitor measures the patient’s response time to catching the device in milliseconds by registering where the stick is released and then grabbed,” explained Richardson.
The patient has about 390 milliseconds from the time that the ReacStick is dropped from standard desk height to register if they should catch the device or not.
This compares closely to the estimated 350 milliseconds a patient has to initiate a recovery strategy after an event, such as a trip that could become a fall.
After the practice rounds the ReacStick mode is changed to Reaction Accuracy.
Reaction Accuracy demands that the brain prevent the automatic urge to catch the device, recognize light illumination status and remember to let the device continue to fall when the light does not appear.
The provider will inform the patient to only catch the stick when they see lights on the top of the monitor turn green.
If the lights don’t turn green, which occurs randomly, the patient should allow the ReacStick to drop to the floor.
“This assessment is done 20 times with the provider keeping track of how many times the patient appropriately caught or dropped the ReacStick,” said Richardson.
In the ReacStick assessment, Simple Reaction Time is ideally under 200 milliseconds, and Reaction Accuracy is ideally greater than 75%.
Lateral plank
Finally, the patient is asked to lay on their side and hold a lateral plank for as long as they can.
This final test observes the patient’s core strength, which is a powerful aid in allowing the patient to catch themselves once they recognize a fall is happening.
The ideal length of time for a lateral plank is about 20 seconds or more.
According to Richardson, patients don’t necessarily need to pass all three tests to be at a lower risk of falls.
“Passing all three of the evaluations is optimal but passing at least two out of the three tests suggests that the patient has the capacity to quickly engage their brain, recognize a serious fall event and change their muscle pattern to prevent the fall or fall in a way that will cause minimal damage,” said Richardson.
“These tests allow us to see where a patient’s areas of weakness are and make rational recommendations to strengthen these or suggest strategies to adapt to them.”
Richardson and his team are continuing to use these methods of assessment in their JEDII Fall Clinic.
The team sees patients that are identified as at risk of falling and through evaluation of clinical tests which represent discrete physiologic abilities in key areas determine why the patient has difficulty balancing on one foot and is at increased fall risk and offer recommendations for improvement or accommodation to the patient’s specific limitations.
“We hope that armed with this information patients will be able to avoid an injury due to a fall and live longer with a better quality of life,” said Richardson.
Additional authors: Stephen R. Lord and Kim Delbaere from the Neuroscience Research Australia, University of New South Wales, Sydney, Australia. James A. Ashton-Miller from the Department of Mechanical Engineering, University of Michigan, Ann Arbor, MI, USA.
Paper cited: “Clinical estimates of three physiologic capacities explain a majority of unipedal stance time,” Aging Clinical and Experimental Research. DOI: 10.1007/s40520-025-03164-8
Sign up for Health Lab newsletters today. Get medical tips from top experts and learn about new scientific discoveries every week.
Sign up for the Health Lab Podcast. Add us wherever you listen to your favorite shows.

Health Lab
Explore thousands of health news & research stories by visiting the Health Lab homepage for more.
Media Contact

Public Relations
Department of Communication at Michigan Medicine
In This Story

James K Richardson
Professor
Stay Informed
Want top health & research news weekly? Sign up for Health Lab’s newsletters today!
Featured News & Stories

Early instruction in scientific reasoning skills can help teens develop greater health literacy and confidence

What’s the latest on 7-OH and kratom availability and addiction care?

Many young adults may not be ready to manage their own health care

Scientists discover that bacteria use an understudied polymer found in all life to protect cell functions during stress

The hidden life of parasites like Cyclospora