Researchers find significant differences in care of life threatening shock after heart attack
The study evaluated cardiogenic shock cases seen across Michigan hospitals between 2018 and 2024
2:00 PM
Author |
Among patients who are treated for the deadliest heart attacks, up to 1 in 10 go into cardiogenic shock, meaning their organs do not get enough blood and begin to fail.
Despite many advances in treating the initial heart attack, cardiogenic shock still kills around half of patients within 30 days.
Most hospitals don’t see many cardiogenic shock patients.
When they do, providers often do not have a standardized way of treating them, according to a study led by Michigan Medicine.
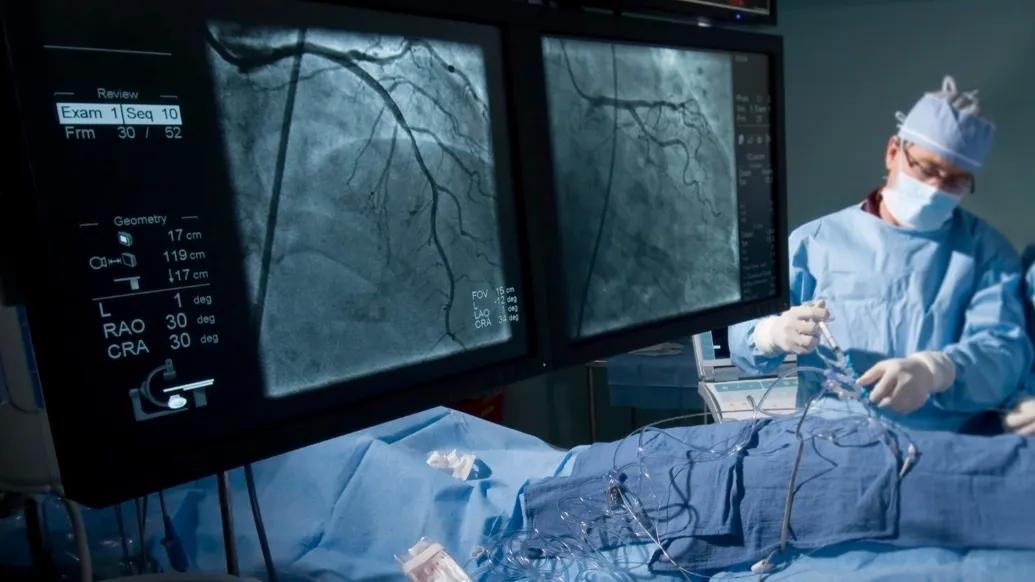
“These are the sickest patients that everyone in the catheterization lab remembers,” said Eric Cantey, M.D., lead author and assistant professor of internal medicine-cardiology at University of Michigan Medical School.
“It takes effective team effort to keep them alive — from the emergency department to the cath lab and the intensive care unit. Our findings highlight that each hospital in the state of Michigan sees these cases infrequently, as well as an extreme variability in the way cardiogenic shock is treated. This presents risks for improving care of patients with this deadly condition.”
Using a statewide database from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium, researchers analyzed nearly 25,000 cases of the most severe kind of heart attack, ST-elevation myocardial infarction, commonly known as a STEMI, seen at 50 different Michigan hospitals between 2018-2024.
STEMI occurs when a major artery that feeds the heart is completely blocked, causing irreversible damage to the heart muscle which can weaken the heart.
Just over 2,000 of these patients experienced cardiogenic shock after undergoing minimally invasive treatment to open the blockage known as percutaneous coronary intervention, or PCI.
Results published in The Journal of the American College of Cardiology reveal that cardiologists who treated shock patients saw an average of 1 patient every 18 months.
“When hospitals see such few cases of cardiogenic shock during a year, it’s difficult to develop standard practices of care,” said David Hamilton, M.D., co-author and clinical assistant professor of internal medicine-cardiology at U-M Medical School.
“The lack of ongoing experience creates a risk that providers will not be properly trained on certain devices and therapies that optimize survival, which ultimately poses a risk for patient safety.”
Treatment options for cardiogenic shock after STEMI
After PCI, patients with cardiogenic shock require immediate treatment in the intensive care unit. Despite multiple decades of research and innovation, the mortality rate is still significantly high.
They may require several medications, including vasopressors to increase blood pressure and inotropes to temporarily improve the heart’s ability to pump.
However, these medications can increase the workload on a recovering heart. They can also cause life-threatening heart rhythms, and kidney injury, both of which increase the risk of death in cardiogenic shock patients.
Other patients are treated with medical devices that assist or completely replace the heart in pumping blood throughout the body, including:
Extracorporeal membrane oxygenation (ECMO), a critical care machine that bypasses the heart and lungs to pump oxygenated blood to the rest of the body.
Intra-aortic balloon pump, which inflates and pushes blood from the heart to the body
Microaxial flow pump (Impella), a pump that ejects blood from the main squeezing chamber of the heart (left ventricle) to the rest of the body.
In recent years, the microaxial flow pump has gained popularity as a treatment for STEMI-related cardiogenic shock, particularly considering data published in The New England Journal of Medicine in 2024 which showed that the heart pump treatment reduced mortality by over 26%.
However, one-quarter of the patients treated with the microaxial flow pump had device-related complications, such as bleeding, kidney injury and infections.
In the Michigan study, fewer than one-quarter of all patients were treated with the microaxial flow pump. Throughout 50 centers in the state of Michigan, there was significant variation in the type of treatment offered to these critically ill patients.
“This points to the main issue that in Michigan hospitals, and likely across the country, the volume of acute myocardial infarction cardiogenic shock is typically low,” Cantey said.
“Because of this, it is difficult for all team members to feel comfortable with all the facets of AMI-CS care — including early detection of cardiogenic shock, stratifying risk, determining proper treatment plans and managing postoperative ICU care to decrease the risk of device complications.”
Need for best practices, adoption
The Michigan Medicine-led group concluded that establishing and implementing shock protocols may help institutions with fewer resources optimize how they manage the condition.
“It is critical that this is not a one size fits all model, but it is equally important that certain best practices for the multiple stages of cardiogenic shock care — such as early detection, prompt revascularization and support, and proactive intensive unit care — are followed.”
For example, fewer than one-third of the study’s patients received a right heart catheterization. This procedure tests the pressures within the heart and is critical for the risk stratification and management of cardiogenic shock in the cardiac intensive care unit.
The findings also speak to the need to potentially centralize cardiogenic shock care, Hamilton says.
“There is potential to create hub and spoke models, in which catheterization labs could transfer patients to centers with expertise in the critical management of STEMI-related cardiogenic shock and use of devices like the microaxial flow pump,” he said.
“Each institution will need a process to ensure its providers are confident and capable of treating with a microaxial flow pump and other available shock devices.”
Now that there is a device that improves outcomes in select patients with cardiogenic shock, researchers say, it is time to think about real-world implementation to improve patient outcomes and safety.
“While there is a lot of work to be done, we believe that our analysis will set the groundwork for future efforts to further move the needle of survival in this critically ill population,” said Hitinder Gurm, MBBS, senior author and chief medical officer at U-M Health.
“The stakes are incredibly high in this sick population, but the potential to further lower the incredibly high mortality rate is what keeps us motivated.”
Additional authors: Aaron Lopacinski, M.D., Elias J. Dayoub, M.D., both of University of Michigan, Siddharth Gandhi, D.O., of McLaren Northern Michigan, Mir B. Basir, D.O., of Henry Ford Health Care System, Amir Kaki, M.D., Henry Ford-St. John Hospital, Ryan D. Madder, M.D., Devraj Sukul, M.D., both of Frederik Meijer Heart and Vascular Institute, and Milan Seth, M.S., of Blue Cross Blue Shield of Michigan Cardiovascular Consortium (BMC2).
Funding/disclosures: Support for BMC2 is provided by Blue Cross Blue Shield of Michigan (BCBSM) and Blue Care Network as part of the BCBSM Value Partnerships program. Although BCBSM and BMC2 work collaboratively, the opinions, beliefs and viewpoints expressed by the authors do not necessarily reflect the opinions, beliefs, and viewpoints of BCBSM or any of its employees.
Basir has served as a consultant for Abiomed. Kaki has received speaker honoraria from and has served as a consultant to Abiomed.
Paper cited: “Managing Cardiogenic Shock Caused by Acute Myocardial Infarction: Invisible Challenges Revealed in a Statewide Registry,” The Journal of the American College of Cardiology. DOI: 10.1016/j.jacc.2025.02.027
Sign up for Health Lab newsletters today. Get medical tips from top experts and learn about new scientific discoveries every week.
Sign up for the Health Lab Podcast. Add us wherever you listen to your favorite shows.

Health Lab
Explore a variety of health care news & stories by visiting the Health Lab home page for more articles.
Media Contact

Public Relations
Department of Communication at Michigan Medicine
In This Story

Hitinder Gurm
Chief Medical Officer
Related

When a Virus Turns Deadly: What You Should Know About Myocarditis

Her heart stopped more than 25 times. ECMO saved her life
Stay Informed
Want top health & research news weekly? Sign up for Health Lab’s newsletters today!
Featured News & Stories

The Power of Mattering
Emergency EEG study suggests need for faster seizure diagnosis and care options

Blue Cross Blue Shield of Michigan and Michigan Medicine reach contract agreement
Michigan firearm data now available in near real-time
