Reframing the role of medications in chronic pain management
An expert explains why solely relying on pain relievers “disempowers patients, clinicians and the drugs themselves”
2:01 PM
Author |
It was just before bedtime, and I was grinding up some Purple Kush.
In the months following my fibromyalgia diagnosis, this treasured cannabis variety had become a mainstay treatment.
It improved sleep and reduced pain, allowing me to build my new yoga practice and stay employed in my post-college job testing water filters.
The cannabis radiated a musky, sweet smell I associated with relief.
I filled the vaporizer bag and inhaled, anticipating a relaxed journey towards sleep.
Instead, my mind raced.
I grew agitated.
I tossed and turned all night, leaving me exhausted and confused when morning finally came.
I tried again over the next days with the same frustrating results.
I should have realized cannabis might stop helping. After all, a similar pattern had happened before.
Prescribed just after my diagnosis, cyclobenzaprine initially helped with sleep and pain, allowing me to face my workday and start exercising.
However, I quickly grew tolerant, and cyclobenzaprine caused grogginess and cognitive fog that soon outweighed any benefits.
Similarly, for months prior to my diagnosis, ibuprofen had eased my hand pain.
However, one day after taking my usual dose, my heart started pounding.
I sneezed repeatedly and violently, then started having trouble breathing.
My partner raced me to the emergency department.
I walked in and promptly blacked out.
When I came to, my full body hives were being displayed to medical interns as “a classic allergic reaction”.
The attending physician noted that such allergies can develop with chronic medication use.
Fast forward 15 years. Now a pain researcher, I see that my experience is surprisingly common.
Regardless of diagnosis and drug class, medications for pain persisting three months or longer (i.e., chronic pain) often initially provide small to moderate pain relief.
Only a subset of people obtain meaningful long term benefit while others have side effects that outweigh any gains.
Consequently, treating chronic pain solely with drugs is like fighting the Lernaean hydra: lop off one head, two grow back.
Of course, there are evidence-based, non-drug strategies for pain: movement, eating and sleeping well, building strong social networks, cognitive behavioral therapy, and more.
Many such strategies are self-motivated and practice based, requiring time, gumption, education, and any number of equipment, transportation, or human supports.
Unlike medications, they often don’t provide immediate relief.
I no longer take medicine habitually, instead pausing to confirm my readiness to experience both potential relief and side effects. This pause decreased my medication use by helping me understand that oftentimes when I am drawn to medicine, I instead need to rest, move or choose a different activity. Infrequent use reduced my tolerance, giving me heightened effect with lower doses, in turn minimizing side effects.”
In some cases, like improperly paced exercise, they may worsen symptoms, causing this process to feel Sisyphean: struggling to push a massive, unwieldy boulder (i.e., symptoms) up a steep hill only to have it repeatedly slip away.
To make these treatments more useful, we must reconceptualize their roles.
Paraphrasing the physician who diagnosed me, “Medications can help control symptoms, allowing patients to restore function through non-pharmacological approaches.”
Put another way, medications are chemical nudges, allowing adoption or improvement previously unreachable non-drug strategies that build mental, physical and emotional resilience.
This reframing has spiraling consequences.
Rather than feeling hamstrung by mediocre medications, clinicians can engage in patient healing through helping work towards realistic, mutually agreed upon, treatment goals.
For example, instead of reducing pain to 0/10, finding the right nudge to take walks or play with the grandkids.
Clinician acknowledgement of these limitations would set more realistic expectations and open opportunities to discuss other necessary pain management strategies.
Doing so would help patients feel less scared and helpless when medication benefits diminish.
For patients, the chemical nudge lens engenders enhanced reflection around what they are seeking through medication, helping support essential non-drug efforts that occur outside the examination room.
Further, non-drug approaches take time to start working but increase in effectiveness with sustained practice. (As a former violinist, I think of my five-year-old self’s scratchy version of Twinkle Twinkle Little Star versus my flowing rendition of Beethoven’s Romance No. 2 in F Minor as a teenager.)
Consequently, clinicians can help patients deftly overlap the initial—and often strongest—period of medication-based pain relief with the challenging non-drug strategy initiation phase.
With this framework, the treatments aren’t altered, but the context in which drugs are given and intent of use changes.
Personally, I have grown more cognizant of my mindset and physical setting before taking medication, admittedly via frustrating trial and error.
I no longer take medicine habitually, instead pausing to confirm my readiness to experience both potential relief and side effects.
This pause decreased my medication use by helping me understand that oftentimes when I am drawn to medicine, I instead need to rest, move, or choose a different activity.
Infrequent use reduced my tolerance, giving me heightened effect with lower doses, in turn minimizing side effects.
In what feels like an odd turn for a scientist, the chemical nudge lens transformed my view of pain medicines into something sacred: these substances, fashioned through millennia of human ingenuity, allow us to engage with ourselves in previously inaccessible ways.
These effects feel miraculous, but like all miracles, can only go so far.
Even Lazarus resurrected needed to return home, find a livelihood and continue living.
All too often, patients pin hopes for healing on clinicians, abdicating their autonomy to heal independently and ability to effectively engage with pain—a critical way our bodies teach us about ourselves, even if the information is undesirable.
Clinicians often feel bound by feelings of inadequacy for being unable to relieve patient symptoms, which can lead to inappropriate prescribing of whatever drugs the patient wants.
The drugs are hobbled by unrealistic curative expectations, masking what they do offer: an otherwise unavailable window of relief during which change becomes more possible.
The relentless focus on finding “perfect” medications disempowers patients, clinicians and the drugs themselves.
The chemical nudge lens restores power to people and chemical actors alike, enabling a more skillful dance that supports non-drug approaches while permitting the inevitably of pain and creating space for its eventual release.

Health Lab
Explore a variety of health care news & stories by visiting the Health Lab home page for more articles.
Media Contact

Public Relations
Department of Communication at Michigan Medicine
In This Story

Kevin F Boehnke, PhD
Assistant Professor
Stay Informed
Want top health & research news weekly? Sign up for Health Lab’s newsletters today!
Featured News & Stories
When should parents stop tracking their kids' location?

7-OH, kratom and the emerging public health crisis for sale across the country

Shipt gift helps address food insecurity
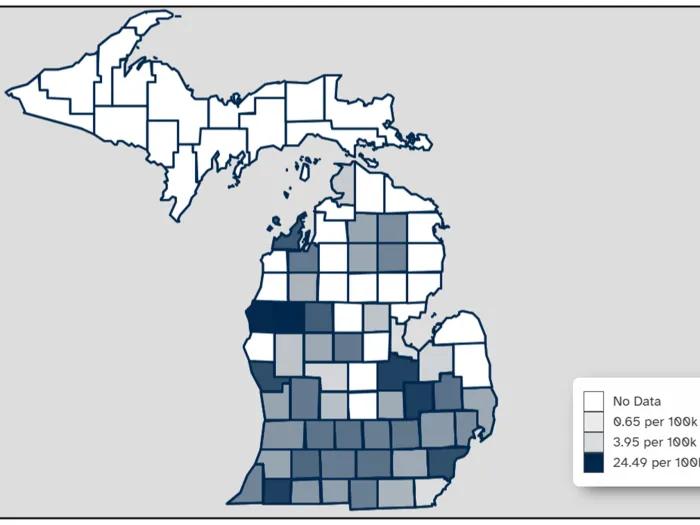
Michigan firearm data now available in near real-time

NASCAR star’s death shows how sepsis can kill anyone if not caught
