U-M cardiologists say anticoagulation clinics still hold a vital role in patient care, even as new drugs claim to reduce the need.
4:12 PM
Author |
Visits to anticoagulation clinics may no longer be part of the routine for patients taking blood thinners for atrial fibrillation or venous thromboembolism.
That doesn't mean, however, the facilities don't serve a purpose.
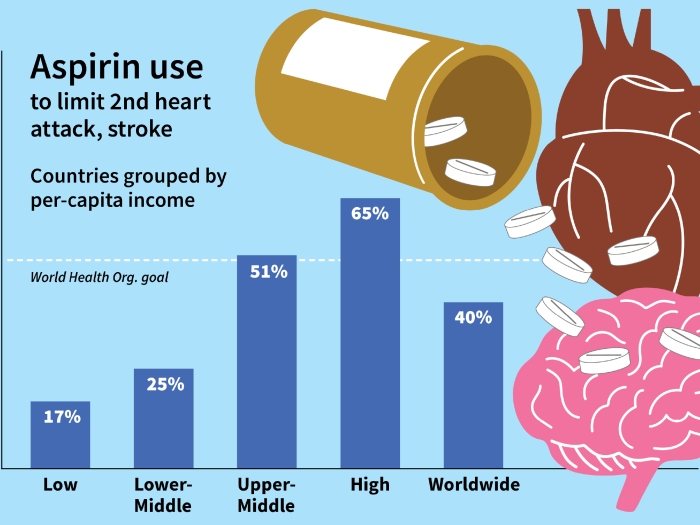
The clinics serve warfarin-treated patients to help monitor and manage the medication. But since 2009, use of direct oral anticoagulants (dabigatran, rivaroxaban, apixaban and edoxaban) has grown as an alternative to warfarin. Much of the marketing around DOACs — the TV ads are hard to miss — emphasize they don't necessarily require frequent clinic visits for monitoring.
"Many wondered if these new drugs would run anticoagulation clinics out of business," says Geoffrey Barnes, M.D., M.Sc., cardiologist and vascular medicine specialist at the University of Michigan Frankel Cardiovascular Center. "But the clinics can have a role no matter what anticoagulant patients are on."
In the American Heart Association's journal Circulation: Cardiovascular Quality and Outcomes, Barnes and colleagues expand the role of traditional anticoagulation clinics and reimagine them as cost-saving medication safety hubs.
He describes three ways the nation's 3,000 clinics can continue serving patients and doctors:
-
Clearing through clutter. Specialty pharmacists and nurses can help select the most appropriate drug and dose from a growing list of anticoagulants, including warfarin, and review with patients how much blood clot prevention will cost. There are fewer diet-drug and drug-drug interactions with DOACs, but there are still some medicines to avoid. "Clinic providers can spend more time with patients than most primary care or specialty physicians," Barnes says. Any prescribing physician will know to check renal function upfront, but long-term monitoring is often overlooked. Clinic providers can establish a regular renal function monitoring plan, and adjust dosage to prevent life-threatening bleeding if renal function declines.
-
Encouraging long-term adherence. This is especially important for DOAC-treated patients, for whom skipping one or two doses may leave them unprotected from a deadly stroke or pulmonary embolism. A recent Veterans Affairs study demonstrated that long-term monitoring of dabigatran treatment by an anticoagulation clinic with support from pharmacists was associated with the highest likelihood for medication adherence. Clinic visits were scheduled at least every three months in major trials comparing warfarin with DOACs. Clinic check-ins have been recommended every three to six months by the European Heart Rhythm Association.
-
Acting as the "go-to team" for periprocedural management. Patients on blood thinners may need to interrupt their anticoagulation therapy when undergoing a teeth cleaning, heart catheterization, colonoscopy or joint replacement. The time needed to stop an anticoagulant before or after a procedure varies greatly depending on medication, a patient's renal function and the bleeding risk of the procedure. "I've seen patients try to coordinate opinions from multiple providers, potentially from different health systems, and it's a struggle," Barnes says. An anticoagulation clinic can help with answers and coordination.
Clinics as safety centers
Beyond the care of patients taking anticoagulants, the existing anticoagulation clinic infrastructure could be leveraged to serve as medication safety clinics for patients taking other potentially dangerous cardiovascular medicines, the authors say.
Patients taking mineralocorticoid receptor antagonist for hypertension or heart failure could be monitored for potassium and renal function. Recent studies have shown that only half of patients taking amiodarone receive the recommended liver and thyroid screening. Both groups of patients could be followed at a medication safety clinic.
Despite the examples and opportunities, the authors believe the greatest barrier to reimagining the anticoagulation clinic is cost. As use of DOACs increases, it might be tempting to discourage use of anticoagulation clinics and avoid paying for these services.
"But we have to remember why the clinics were created in the first place: to reduce bleeding risk and avoid stroke and pulmonary embolism," Barnes says. "When we reduce these complications we've improved health care's bottom line."

Explore a variety of healthcare news & stories by visiting the Health Lab home page for more articles.

Department of Communication at Michigan Medicine
Want top health & research news weekly? Sign up for Health Lab’s newsletters today!