Breakthroughs in the field of genomics are revolutionizing prevention, diagnosis, and care
Author |

In the last 20 years, the scientific community has made remarkable strides in diagnosing, treating, and even curing cancer. Cancers that were considered a death sentence two generations ago are now treatable, with patients surviving for years, and some types of cancer can be cured without requiring patients to go through chemotherapy.
But the job isn't done. This year, 1,918,030 new cancer diagnoses and 609,360 cancer deaths are projected to occur in the United States, according to the American Cancer Society.
Researchers at the U-M Rogel Cancer Center are leading the charge in finding the molecular mechanisms behind cancer and working to identify and help individuals with genetic predisposition to cancer. Detailed evaluation of the genetic make-up of cancer is leading to more targeted treatments, which means longer survival and better quality of life. At the same time, genetic testing can help identify those at greatest risk of developing cancer, enabling more interventions to prevent cancer or detect it in an earlier, more treatable phase.
Some of this groundbreaking work began in 1956, when James V. Neel, M.D., Ph.D., founded the Department of Human Genetics at U-M, which was the first department of its kind in the country. The Rogel Cancer Center was also one of the first cancer centers to perform comprehensive sequencing of advanced cancer tumors, looking at DNA, RNA, and other genetic components. A panel of experts in precision oncology — researchers and clinicians — uses this information to understand what's driving cancer and recommend the best way to treat it.
Eric Fearon, M.D., Ph.D., the Emanuel N. Maisel Professor of Oncology and director of the Rogel Cancer Center, compares it to car repairs. Today, fixing a car no longer means popping the hood and hoping to spot the problem. "When you take a modern car into the shop, they plug it into the computer, and it says what diagnostic trouble codes are present," he says. "By sequencing the cancer genome, you can actually know the trouble codes that are wrong. It doesn't mean you know how to fix the issues or have the parts in the shop, but you know what's causing the problem, and perhaps the best repair options."
Before a Cancer Diagnosis
A molecular approach to cancer can also spot those trouble codes before anything goes wrong. Genetic screening can help identify those at high-risk of developing cancer based on inherited genetic factors, including people with cancer who are at risk for additional cancers.
But a Michigan Medicine study published in 2018 found nearly half of recently diagnosed breast cancer patients who were eligible for genetic testing didn't get it, and a quarter of these patients were not counseled about the potential for genetic predisposition.
"We know that there are certain people who would benefit tremendously from special cancer prevention interventions because they have genetic susceptibility to cancer," says Elena Martinez Stoffel, M.D., MPH., associate professor of internal medicine and director of the Rogel Cancer Center's Cancer Genetics Clinic. "Right now, we do a really poor job of identifying these people before their cancer diagnosis."
Genetic testing of people who have already been diagnosed with cancer can also identify potential risk for those patients' family members. Yet it's been challenging to trickle down genetic counseling to these potentially vulnerable relatives.
In 2020, Michigan Medicine was awarded a $4 million grant from the National Cancer Institute for a five-year project to increase rates of genetic testing among cancer patients with personal or family histories that suggest risk for hereditary cancer syndromes. The project is a collaboration between the Rogel Cancer Center and the Michigan Oncology Quality Consortium, a statewide network of oncology practices focused on improving the value and quality of cancer care in Michigan. Researchers will implement a family health survey for cancer patients statewide to help clinicians identify those who meet the criteria for genetic testing.
"If we can make the diagnosis of a hereditary cancer syndrome at the time of their cancer diagnosis, the information could have implications not only for their own cancer treatment but also for cancer prevention for members of their family," Stoffel says.
By understanding their genetic predisposition to cancer, people can pursue more frequent screening or prevention strategies to reduce their risk or detect cancer in an early, more treatable stage.
During a Cancer Diagnosis
Once cancer develops, genomic sequencing has led to breakthroughs in how patients are treated and opened doors to new avenues of research.
Michigan's Oncology Sequencing Program (MI-ONCOSEQ) began in 2010, making it one of the first in the nation. The program goes far beyond the capability of commercially available genetic testing kits, which look at about 150 genes. MI-ONCOSEQ reviews more than 1,700 genes. Since launching, MI-ONCOSEQ has sequenced more than 4,000 patients' tumors.
Among patients with advanced cancer whose therapy was informed by sequencing results, nearly 40% experienced some clinical benefit from that treatment and 20% experienced exceptionally good responses, according to a paper published in JAMA Oncology in 2021. Another study, published in JAMA in 2015, found genetic sequencing changed the course of treatment in 46% of pediatric cancer cases at Michigan Medicine.
"Now that we have the opportunity to comprehensively analyze, at a molecular level, the basis of an individual's cancer, we have a chance to better understand the combination of molecular drivers in that particular patient," says Arul Chinnaiyan, M.D., Ph.D., the S.P. Hicks Endowed Professor of Pathology and Urology and director of the Michigan Center for Translational Pathology. "The thought is that by having a deep understanding of all the drivers of a patient's cancer, you can create individual treatments and have a better chance at curing that patient."
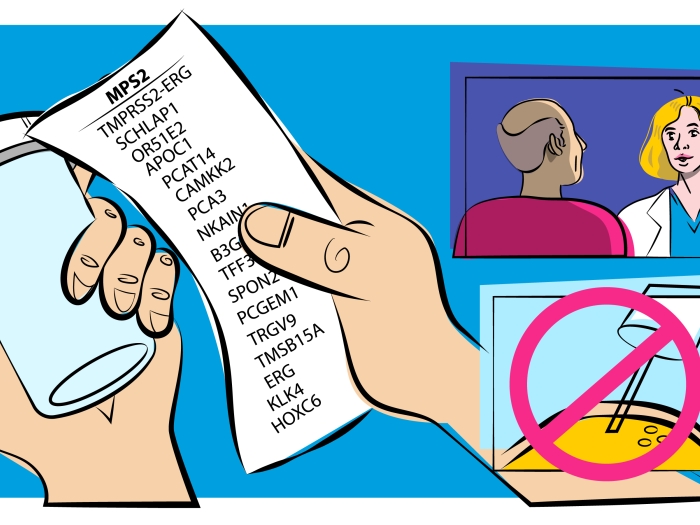
Chinnaiyan was recently awarded the Sjöberg Prize by the Royal Swedish Academy of Sciences for his discovery of a recurrent gene fusion in prostate cancer, which has led to a better understanding of how prostate cancer develops and new methods to detect the disease.
After a Cancer Diagnosis
Despite strides in reducing cancer mortality rates, some cancers don't respond to treatment, or they grow resistant to it. For example, small cell lung cancer has a 7% five-year survival rate, according to the American Cancer Society, and certain types of breast, ovarian, and prostate cancer are considered very difficult to treat right now.
But the definition of "difficult to treat" has already changed, again thanks to genomic sequencing.
In a 2017 study presented at the American Society of Clinical Oncology annual meeting, Michigan Medicine researchers showed that 72% of patients with advanced cancer could be referred for a potential targeted treatment based on a genetic marker found in their tumor. While most patients weren't able to enroll in those trials (their cancer was too advanced, they were too sick, or they couldn't travel to the trial site location), 11% did, says Erin Cobain, M.D., assistant professor of internal medicine and lead author of the 2021 JAMA Oncology paper that built on the results of the 2017 study.
Michigan Medicine is also using genomic sequencing, along with the American Society of Clinical Oncology's Targeted Agent and Profiling Utilization Registry (TAPUR) study, to find new treatment options for patients with advanced cancers that aren't responding to typical drugs and treatment.
TAPUR takes genomic sequencing from tumors with a large number of mutations and assesses whether cancer drugs previously approved for one type of cancer might also help patients with different cancer types, if they have the same specific alterations to tumor DNA and RNA.
One example is in breast cancer, where immunotherapy has proven largely ineffective. But a trial that ran from 2016 to 2018 at Michigan Medicine and other sites enrolled 28 women with advanced breast cancer whose tumors had molecular changes often seen in types of cancers that respond to immunotherapy. Of those women, one-third had their tumors controlled with the immunotherapy drug pembrolizumab, and a handful saw benefits lasting more than a year.
U-M researchers are also using information from genomic sequencing to look at alterations across different kinds of cancers, and enrolling patients in "basket trials," where those with different kinds of cancers but the same gene alterations are put into one "basket" and tested to see if a drug targeting the alteration works for them. So a prostate cancer patient and breast cancer patient may end up in the same basket, receiving the same drug.
"In some cases, drug companies take the FDA approval path focused on a specific disease in a specific group of patients," says Joshi Alumkal, M.D., the Wicha Family Professor of Oncology and professor of internal medicine. His research focuses on patients with aggressive, advanced prostate cancers, which often share genetic mutations found in other types of aggressive cancer. "We are learning lessons from other diseases, such as small cell lung cancer, to understand how alterations in specific genes can also make certain prostate cancers more deadly," says Alumkal. This type of cross-disease research may lead to basket trials that focus on identifying tumors that start out from different organs but that harbor similar genetic alterations that may be targeted with the same drug, instead of taking a more organ site-focused approach.
While these advances haven't affected a huge number of patients yet, it's just the start of exploring the possibilities of advanced genomic sequencing in cancer care, says Cobain. "We need to think about how we can move this to earlier in the cancer treatment process, and keep working to expand access and bring it to more people."

The Future of Cancer
Learning more about the complex drivers of cancer can help create new drugs and targets for treatments, but it also shows how much researchers don't know about the many subsets of this disease. Each new study is like opening a Pandora's box that holds both hope and chaos.
Chinnaiyan believes the biggest advancements in new therapy development are still to come. "As time moves forward, we're going to have a better chance at potentially developing drugs against these so-called 'undruggable' cancers," he says.
While immunological therapies work for some cancer patients, they do not work for everyone, says Chinnaiyan. Those treatments take advantage of the immune system to hit at one factor driving cancer in that patient, but it's "relatively rare to have a single driver in a tumor. More often, cancer will have five to ten drivers. How do you treat all of those? And how do you run a clinical trial for five or six drugs, and manage the toxicity level in patients?"
Researchers are also thinking differently about how to look at cancer samples. In her work, Sofia Merajver, M.D., Ph.D., the Greater Good Breast Cancer Research Professor, professor of internal medicine, and director of the Breast and Ovarian Cancer Risk and Evaluation Program, has been going beyond studying tumor samples to further expand what researchers know about cancer. Her lab is developing a platform that takes a tumor sample and uses 3D simulations to grow those samples and "see how the tumor was growing a few days ago when it was still in the patient's body." They then expose that tumor to up to 100 or more drugs over a period of five to seven days to see how it responds.
"The goal of the program is to develop a reliable and accurate way to assess what drugs or combinations of drugs stand a chance to kill active, live cancer cells," she says. The live part is crucial to their work. "All of our current technologies essentially take a snapshot of a tumor biopsy, so all the cells are dead. There's absolutely no way to evaluate any aspect of the cells, whether they are cancer cells or normal, that is helping or hurting the cancer's growth."
Merajver believes that science will get to the point where it can detect cancer cells far earlier than current methods, especially when taking into account non-genetic factors that promote cancer development. "In 30 years, we are going to have the capability of doing molecular ascertainment of early changes that are causing cancer to occur in normal tissues. Some of these changes are happening as early as our teens, or in our 20s, and then we get cancer in our 50s," she says. She envisions those check-ins being done by simple blood, saliva, or urine tests to detect changes in a few cells before they proliferate.
"In the future, we'll be able to monitor those changes early when they affect just a few cells. That doesn't mean all of a sudden you'll get chemotherapy for it, because you don't have the disease, but you'll know that your body is poised to make cancer because of these changes" — and can start other potential preventative treatments for it that researchers haven't realized yet.